[ad_1]
By Lambert Strether of Corrente.
Readers who’ve been following our HICPAC journey (CDC’s Healthcare An infection Management Practices Advisory Committee) can be conscious that HICPAC is holding a gathering on August 22 that might presumably decrease an infection management requirements, particularly by eliminating any chance of common masking with N95 respirators in hospital settings. (HICPAC members are all affiliated with hospitals or different medical amenities, and are thus conflicted about recommending towards common masking in hospital amenities when their very own establishments have already achieved so.) Readers can even bear in mind that one motive HICPAC downgraded protections towards airborne MRSA in hospitals was budgetary (and never affected person security). Lastly, readers can be conscious that HICPAC is out of compliance with each the letter and the spirit of the Federal Advisory Committee Act (FACA), the legislation that governs Federal advisory committees.
On this submit, I’ll strategy what I hope is the delicate underbelly of the beast: a draft doc entitled “Isolation Precautions Guideline Workgroup,” acquired by HealthWatch USA after HICPAC’s earlier assembly on June 8, not obtainable on the CDC’s HICPAC web page, regardless of its standing as a “work group” document. From Slide 2 of that doc:]
")
I write “Slide” 2 as a result of, in yet one more signal of our society’s operational incapability, HICPAC is making selections affecting the well being and lives of hundreds of thousands not solely primarily based on a draft, however a draft PowerPoint presentation, bullet factors and all. That mentioned, from the Common Companies Administration (GSA), the FACA steerage on “deliberative materials”:
The Federal Advisory Committee Act requires advisory committees to make obtainable for public inspection written advisory committee paperwork, , working papers and research.
For my part, HICPAC’s Designated Federal Officer, Michael Bell, M.D., ought to use his authority to both postpone or instantly adjourn the August 22 assembly, reconvening when HICPAC is totally compliant with FACA.
Be that’s it could, on this submit I’ll have a look at one part of the “Isolation Precautions” draft: “The Proof Evaluation” (beginning on Slide 26), which poses the next query:
For healthcare personnel caring for sufferers with respiratory infections, in stopping an infection?
The “Proof Evaluation” solutions to the query it poses — spoiler: “No,” however they’re unsuitable — within the type of aggregated tables (“snapshots”) characterizing many masks research. First, I’ll study the strategies by which these tables have been created. Then, I’ll disaggregate the tables, which can yield some attention-grabbing outcomes. (It’s maybe at this level evidently that each the strategies and the tables are positively replete with FACA violations, and actually, at essential factors, opaque.) Each elements are fairly detailed. This submit can be lengthy, however the issues that fulfill solely come actual gradual.
Earlier than I start, a observe on the scope of this submit: The “Proof Evaluation” additionally raises the equation of “Hostile Results” from masking — right here one remembers WHO masks maven John Conly weighing the harms of SARS-CoV-2 an infection towards the harms of zits — however they’re out of scope for this submit. Additional, although the “H” in HICPAC stands for “Healthcare,” not “Hospital,” I’ll prioritize hospitals over different establishments; partly as a result of I want to drive the mission of common masking in hospitals ahead, but in addition as a sop to the pursuits of HICPAC members, the overwhelming majority of whom are affiliated with these establishments.
HICPAC “Proof Evaluation” Strategies (with FACA Violations)
Slide 28 offers an outline of the strategies used for the “Proof Evaluation”:
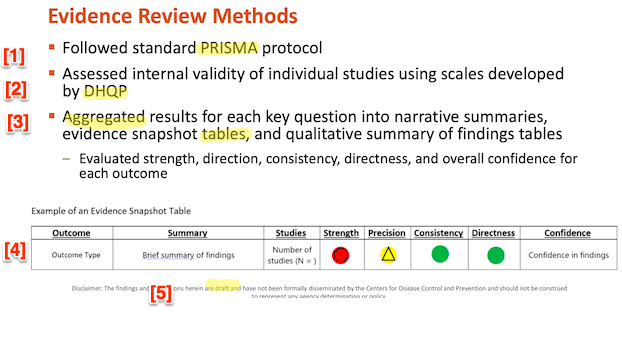
First, I’ll have a look at PRISMA [1], then DHQP [2]. I’ll have a look at the aggregated tables [3] within the subsequent part, disaggregating the so-called “proof snapshots.” Word as soon as extra the boilerplate at [5]: Whether or not or not “the findings and conclusions herein are draft” and “haven’t been formally disseminated by the Facilities for Illness Management and Prevention and shouldn’t be construed to symbolize any company dedication or coverage,” that this doesn’t take away HICPAC’s obligation beneath FACA to make this draft obtainable to the general public. (I’ve gotta say that the purple, yellow, and inexperienced icons remind me powerfully of the color-coded “Homeland Safety Advisory System” beneath President George W. Bush. Crimson is dangerous!)
First, PRISMA. Prisma (“Most popular Reporting Objects for Systematic Opinions and Meta-Analyses”) is sponsored by the Ottawa Hospital Analysis Institute, the College of Oxford, and Monash College. PRISMA’s scope:
PRISMA is an evidence-based minimal set of things for reporting in systematic critiques and meta-analyses. PRISMA primarily focuses on the reporting of critiques evaluating the results of interventions, however may also be used as a foundation for reporting systematic critiques with goals aside from evaluating interventions (e.g. evaluating aetiology, prevalence, analysis or prognosis).
Properly and good. PRISMA additionally gives a guidelines for entities that want to affirm to its pointers. Right here, in related half, is the guidelines; it’s a literal guidelines; I’ve helpfully added a purple “❌” in the best hand column for each merchandise that’s not supplied by the HICPAC “Proof Evaluation”:
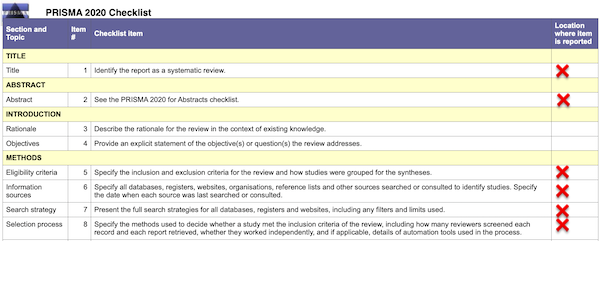
Intimately by merchandise # (column 2):
(1): The “Proof Evaluation” shouldn’t be recognized as a “Systematic Evaluation.” That phrase seems nowhere within the doc.
(2): There is no such thing as a summary.
(5): The inclusion and exclusion standards for the research usually are not specified. (The Appendix comprises all of the masks research listed within the “References” formatted as a desk. I’ve made all hyperlinks clickable, one thing HICPAC unaccountably did not do.)
(6): No data sources are specified. No dates for search or session are specified.
(7): No “full” search technique is offered.
(8): No choice technique is specified.
In brief, we’re taking a look at a imprecise gesture in PRISMA’s path, not “customary PRISMA protocol,” as Slide 28 would have it. We’re not trying on the “minimal set” of things essential to observe PRISMA pointers. If a guidelines with the lacking gadgets doesn’t exist, then HICPAC is derelict in its duties. If it does exist, even in draft type, then HICPAC is in gross violation of FACA by not making them public. In both case, we’re trying mere formalism.
Second, DHQP (CDC’s Division of Healthcare High quality Promotion). From its web page:
The mission of the Division of Healthcare High quality Promotion (DHQP) is to guard sufferers; defend healthcare personnel; and promote security, high quality, and worth in each nationwide and worldwide healthcare supply programs
And:
In finishing up its mission, DHQP… promotes the nationwide implementation of Healthcare An infection Management Practices Advisory Committee (HICPAC) suggestions and different evidence-based interventions to forestall HAIs, antibiotic resistance, and associated antagonistic occasions or medical errors amongst sufferers and healthcare personnel.[1]
Properly and good. However the place, precisely, are these “scales” (Slide 28, above) developed by DHQP, by which the “inner validity of particular person research” aggregated within the putative “Proof Evaluation” is assessed? The scales usually are not included wherever within the draft doc, not even by reference. Because the creator of the “Proof Evaluation,” “Erin Stone, MPH” is the “Lead, Workplace of Tips and Proof Evaluation (OGER)” IN DHQP, one presumes the scales exist and have been utilized to the research. As soon as once more, if these deliverables don’t exist, HICPAC and derelict in its duties. In the event that they do, even in draft type, HICPAC is in gross violation of FACA.
Having established that the “Proof Evaluation” doesn’t conform to PRISMA, and having established that if certainly there are “scales” by which the aggregated research have been evaluated, we the general public do not know what they could be or the place they’re to be discovered — not on the HICPAC web page! — allow us to flip to the “snapshot tables” and disaggregate them.
High quality of HICPAC Proof Evaluation on Masks
There are two “snapshot tables” aggregating the person research (recalling that I’ve dominated “Hostile Occasions” out of scope). Allow us to have a look at every in flip. Slide 31:
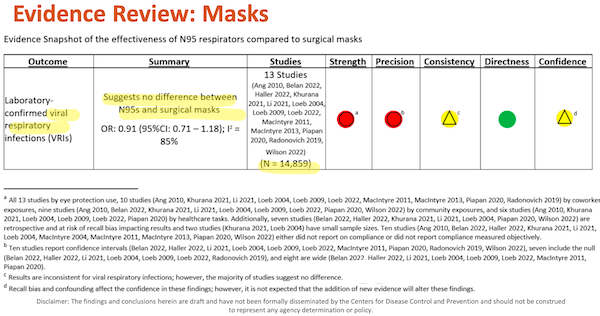
I’ve helpfully highlighted main factors in yellow. Below “Consequence,” we see that this desk is straight related to Covid, which is airborne. Below “Abstract” we see how DHQP, within the individual of Erin Stone, has answered the foremost query posed by the “Proof Evaluation.” Below Research, we see “N”, presumably the aggregated N of all of the research. (I spotlight this solely as a result of it appears odd to view individuals throughout research as fungible; maybe statistics or epidemiology professionals can make clear.)
Now let’s have a look at the footnotes to the desk, (d) – (a), as a result of as any lawyer is aware of, footnotes are the place the enjoyable is available, and as Edward Tufte is aware of, the element is buried on the lowest stage.
(d) “Recall bias and confounding of those findings; nevertheless, that the addition of latest proof will alter these findings.” First, “have an effect on the boldness” how a lot? Apparently, that is totally a subjective matter, very similar to “confidence” within the inventory market, and never a metric in any respect. So we don’t want to fret very unduly about statistical element, if DHQP doesn’t. Subsequent, observe the institutional voice in “it’s not anticipated.” “Not anticipated” by whom and why? As soon as once more, FACA wish to know, particularly since HICPAC is about to resolve not to attend for “new proof” (that’s, extra research, maybe like this one) earlier than making a call affecting the life and well being of hundreds of thousands.
(c) “Outcomes are ; nevertheless, the vast majority of research recommend no distinction.” First, “inconsistent” why? The Covid aware wish to know. Second, is science actually carried out by majority vote? MR SUBLIMINAL Pause for dialogue of paradigm shifts and “one funeral at a time”.
(a) – (b) Metrics for “Energy” and “Precision” are disaggregated in Desk I under.
Slide 32:
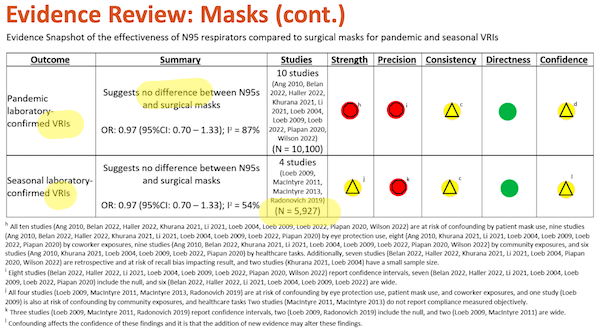
As soon as once more, I’ve highlighted main factors in yellow. Below “Consequence,” we see “VRI” (Viral Respiratory An infection, which is sweet, since SARS-CoV-2 is a virus). For feedback on “Abstract” and “Research, see Slide 31, above.
And to the footnotes, once more ranging from the underside:
(l) “Confounding impacts the boldness in these findings the addition of latest proof .” First, “and it’s that” exhibits that this footnote, not being grammatical is meaningless; learn it once more for those who disagree. Second, “might alter these findings” why? Who says? And why does does Slide 31, footnote (d) “not count on” new proof, and this footnote ponder it?
Now allow us to disaggregate. Desk I lists each examine within the “snapshots” in Slides 31 and 32. My purpose in doing that is to see if the research differ considerably in any method, such that an aggregation would conceal relatively than reveal. (Recall from our examination of PRISMA that we have no idea the inclusion or exclusion standards for the research, the data sources or dates of search, the search technique, or the choice technique.) First, I’ll current the disaggregation, then clarify it, then have a look at what the aggregation might have hid.
Desk I: Disaggregating HICPAC’s “Proof Evaluation” on Masking
| Energy | Precision | ||||||||||||
| Confounders | |||||||||||||
| # | Quick Identify | Examine Sort | Demerits | Eye | Coworkers | Pnt. Masks | Commun. | Duties | Retro. | Small | Compl. | CI | Null |
| 26 | Macintyre 2011 | RCT | 2 | ` | ❌ | ✅ | ❌ | ||||||
| 27 | Macintyre 2014 | RCT | 2 | ❌ | ❌ (2004) | ❌ | ❌ | ||||||
| 39 | Radonovich 2019 | RCT | 2 | ❌ | ❌ | ✅ | ✅ | ||||||
| 28 | Macintyre 2013 | RCT | 3 | ❌ | ❌ | ❌ | ❌ | ❌ | |||||
| 14 | Haller 2022 | Cohort | 4 | ❌ | ❌ | ❌ | ❌ | ✅ | ✅ | ||||
| 7 | Belan 2022 | Matched case-control | 5 | ❌ | ❌ | ❌ | ❌ | ❌ | ✅ | ✅ | |||
| 24 | Loeb 2009 | Randomized Trial | 5 | ❌ | ❌ | ❌ | ❌ | ❌ | ✅ | ✅ | |||
| 23 | Loeb 2022 | Randomized Trial | 5 | ❌ | ❌ | ❌ | ❌ | ❌ | ✅ | ✅ | |||
| 21 | Li 2021 | Cohort | 6 | ❌ | ❌ | ❌ | ❌ | ❌ | ❌ | ✅ | ✅ | ||
| 46 | Wilson 2022 | Cross-sectional | 6 | ❌ | ❌ | ❌ | ❌ | ❌ | ✅ | ❌ | |||
| 36 | Piapan 2020 | Observational | 7 | ❌ | ❌ | ❌ | ❌ | ❌ | ❌ | ❌ | ✅ | ❌ | |
| 5 | Ang 2010 | Observational | 8 | ❌ | ❌ | ❌ | ❌ | ❌ | ❌ | ❌ | ❌ | ||
| 25 | Loeb 2004 | Cohort | 8 | ❌ | ❌ | ❌ | ❌ | ❌ | ❌ | ❌ | ❌ | ✅ | ✅ |
| 17 | Khurana 2021 | Observational | 10 | ❌ | ❌ | ❌ | ❌ | ❌ | ❌ | ❌ | ❌ | ❌ | ❌ |
LEGEND
Aside from “#”, column headings are derived from Slide 31:
#: Cross-reference to “#” column in Desk II, within the Appendix.
Confounders: “Eye,” Eye Safety; “Co-Staff,” Co-Employee Exposures; “Pnt. Masks,” Affected person Masking; “Duties,” Healthcare Duties.
Retro.: Retrospective, prone to recall bias.
Compl.: Both didn’t report on compliance, or didn’t measure objectively.
CI: Confidence Interval
Null: Contains the null speculation.
Studying horizontally, you’ll be able to see that each row represents a examine. In every row, there are columns for all of the confounders and different adverse elements (“Retro.”, “Small”) described in footnotes (a)-(b) in Slide 31, and footnotes (h)-(okay) in Slide 32. Wherever a footnote categorized a examine with a adverse issue, I put a purple “x” in that column. For every examine, I summed the purple “x”‘s, and put that worth within the Demerits column. I then sorted the desk on Demerits. As you’ll be able to see, research 26 – 39 have the fewest demerits — therefore are the most effective research, for this definition of “greatest.” Examine 17, on the backside, with demerits throughout the board, is the worst.
What does our disaggregation present? Let’s quote from the “greatest” research, which I’ve highlighted. (It might or is probably not vital that 4 out of the highest 5 are [genuflects] RCTs.) There are three Macintyres, so let’s quote from them first:
First, #26, Macintyre 2011, “A cluster randomized scientific trial evaluating match‐examined and non‐match‐examined N95 respirators to medical masks to forestall respiratory virus an infection in well being care employees.” From the Interpretation:
p. A good thing about respirators is recommended however would have to be confirmed by a bigger trial, as this examine might have been underpowered.
Word that the “Proof Evaluation” does not characterize Macintyre 2011 as “small,” so maybe Macintyre is being overly punctilious (they make a lot of different {qualifications}, as they need to, within the dialogue). N = 1441 HCWs in 15 Beijing hospitals. An attention-grabbing sidelight on antagonistic occasions:
Apparently, this inhabitants of Chinese language HCWs reported general comparable charges of discomfort with masks as mother and father in our family examine, 10 with greater charges within the N95 group, however it didn’t have an effect on their adherence with masks/respirator carrying. This implies that discomfort shouldn’t be the first driver of adherence, and relatively, cultural acceptability and different behavioural elements could also be the primary motive for non‐adherence. The previous expertise of Beijing well being employees with SARS might also be an element within the excessive adherence. This stage of adherence might not translate to Western cultural contexts in a standard winter season, particularly for N95 respirators; nevertheless, adherence can change with notion of threat.
Second, #27, Macintyre 2014, “Efficacy of face masks and respirators in stopping higher respiratory tract bacterial colonization and co-infection in hospital healthcare employees“:
towards bacterial colonization, co-colonization and viral-bacterial co-infection. We confirmed that twin respiratory virus or bacterial-viral co-infections will be lowered by way of N95 respirators. This examine has occupational well being and security implications for well being employees.
And:
We’ve beforehand proven that N95 respirators defend towards scientific respiratory sickness (MacIntyre et al., 2011, Macintyre et al., 2013). N95 respirators, however not medical masks, have been considerably protecting towards bacterial colonization, co-colonization, viral-bacterial co-infection and twin virus an infection in HCWs. We additionally confirmed a statistically vital lower in charges of bacterial respiratory colonization with rising ranges of respiratory safety. The bottom charges have been within the N95 group, adopted by the medical masks group, and the best charges have been in HCWs who didn’t put on a masks. Though the scientific significance of this discovering is unknown when it comes to the implications for HCWs, we have now proven that such colonization will be prevented by way of N95 respirators.
Third, #28, Macintyre 2019, “A Randomized Medical Trial of Three Choices for N95 Respirators and Medical Masks in Well being Staff“:
. Most insurance policies for HCWs suggest use of medical masks alone or focused N95 respirator use. Steady use of N95s resulted in considerably decrease charges of bacterial colonization, a novel discovering that factors to extra analysis on the scientific significance of bacterial an infection in symptomatic HCWs. This examine gives additional information to tell occupational coverage choices for HCWs.
And:
In a setting of excessive occupational threat for HCWs, the important thing statement of this examine is important protecting efficacy towards scientific an infection of steady use of N95 respirators in contrast with focused use and medical masks, regardless of considerably poorer adherence within the steady use N95 arm. These outcomes add weight to the findings of our earlier examine (16) that confirmed that N95 respirators have superior scientific efficacy to medical masks, regardless of the higher discomfort and decrease adherence related to respirator use. We additionally confirmed that the good thing about N95 respirators persevered after adjusting for the potential confounding by influenza vaccination and hand washing.
(An attention-grabbing dialogue follows on why a management arm with no masking isn’t moral, not less than in China.
And now, to be honest, fourth, #39, Radonovich 2019, “N95 Respirators vs Medical Masks for Stopping Influenza Amongst Well being Care Personnel: A Randomized Medical Trial“:
Amongst outpatient well being care personnel, N95 respirators vs medical masks as worn by individuals on this trial resulted in within the incidence of laboratory-confirmed influenza.
And:
On this pragmatic, cluster randomized trial that concerned a number of outpatient websites at 7 well being care supply programs throughout a large geographic space over 4 seasons of peak viral respiratory sickness, there was no vital distinction between the effectiveness of N95 respirators and medical masks in stopping laboratory-confirmed influenza amongst individuals routinely uncovered to respiratory sicknesses within the office.
Lastly, fifth, #14 Haller 2022, “Affect of respirator versus surgical masks on SARS-CoV-2 acquisition in healthcare employees: a potential multicentre cohort“:
from SARS-CoV-2 for HCW with frequent publicity to COVID-19 sufferers.
And:
That is, to our information, the primary potential multicentre examine evaluating the impact of respirators and surgical masks relating to safety from SARS-CoV-2.
The general affiliation between FFP2 use and threat for SARS-CoV-2 an infection was marginally not vital. That is in all probability a mirrored image of the heterogeneous examine inhabitants, two thirds of which consisted of HCW with solely sporadic (and even no identified) COVID-19 publicity. Nevertheless, for HCW with frequent publicity, we discovered a big protecting impact related to FFP2 use. A number of studies recommend that aerosol transmission is certainly a non-negligible mode of SARS-CoV-2 transmission and that respirators might present extra safety in comparison with surgical masks. However, case studies have urged that surgical masks are equal to respirators in defending HCW from SARS-CoV-2 an infection/ These supposedly contradictory findings will be reconciled when contemplating a selected function of SARS-CoV-2, particularly its excessive overdispersion.
Why the variations between Macintyre 2011, Macintyre 2014, and Macintyre 2019, on the one hand (thumbs as much as respirators, thumbs all the way down to “Saggy Blues,” and Radonovich 2019 (“makes no distinction”)? I might speculate that each one the Macintyre research have been for a single season in-hospital, and Radonovich was over a number of years for outpatient websites, so the group was a large confounder. Why the distinction between Radonovich 2019 and Haller 2022, which incorporates hospitals and outpatient clinics (rehabilitation, psychiatry)? I can’t speculate, though Radonovich was for influenza, and Haller for flu.
Conclusion
A number of ideas:
1. I believe any reader or citizen not inside the comfortable membership of HICPAC and DHQP would and of proper must be pissed off and outraged by the dearth of transparency within the course of of constructing masks coverage. FACA was designed, and GSA supplied steerage, precisely in order that the general public may very well be totally knowledgeable of the scientific considering behind HICPAC steerage. And but, as I present in case after case, data that FACA mandates be made “obtainable for public inspection” (together with drafts) is outright lacking, whether or not from the “Isolation Precautions Guideline Workgroup” doc, or from the CDC web site. How is a boring regular like me supposed to arrange for the August 22 HICPAC conferences? Are we merely to take CDC deliverables on religion? How has that been understanding up to now?
2. Readers and residents, if not already outraged by lacking data and HICPAC’s failure to abide by the plain which means of FACA, must also be outraged by HICPAC’s mischaracterization of the fabric that we can see. DHQP characterizes its so-called “Proof Evaluation” as following PRISMA “customary protocol.” As I present, it doesn’t, all the way down to the very title. Once more, if there’s a full, written, formal model of the “Isolation Precautions Guideline Workgroup” parallel to or derived from the slides, it’s a FACA violation to not make it “obtainable for public inspection.” Does it exist? Or a slide desk — is that each one there’s?
3. I’d very very similar to to consider that after I disaggregate Slides 31 and 32, and pro-respirator, anti-Saggy Blue research miraculously float to the highest, that I’ve dedicated an error, and that HICPAC and CDC are on the up-and-up, having realized one thing from CDC’s preliminary debacle on masks coverage, and its shedding tooth-and-nail battle towards the science and engineering of airborne transmission. Recall, nevertheless, our examination of PRISMA: We have no idea the inclusion or exclusion standards for the research, the data sources or dates of search, the search technique, or the choice technique. CDC has type. A hermeneutic of suspicion is totally justified.
4. Grant, for a second, that each one the research are dangerous and we don’t know something. Doesn’t it make sense to err on the aspect of affected person welfare, relatively than Hospital An infection Management’s line merchandise for PPE?
5. “However muh statistics!” What statistics? I don’t see any statistics. I see coloured icons. See dialogue of PRISMA and DHQP, above.
6. Provided that “every thing is like CalPERS,” I’m wondering if HICPAC has merely delegated an excessive amount of authority to employees, and is just rubberstamping DHQP’s work product, not least as a result of its implicit conclusions conform to their very own priors.
NOTES
[1] DHQP “promotes” HICPAC suggestions, HICPAC’s constitution says that considered one of HICPAC’s “duties” is to offer “steerage” to DHQP, and but right here we have now DHQP offering an “Proof Evaluation” to HICPAC. All of it appears relatively reflexive and round.
APPENDIX
Desk II: HICPAC’s”Literature evaluate: Masks References”
HICPAC’s “Literature evaluate” is a listing that begins on Slide 49. For readability, I’ve formatted the record in desk type. Desk is sorted with Masks (“M”) first, then Hostile Occasions (“AE”). Though this submit solely covers masks, all of the references are supplied as a service.
LEGEND
M/AE: Masks, Hostile Occasions.
T/Q/O: Testing, Questionnaire, Different
FT/A: Full Textual content, Summary
It happens to me that a few of the “Gish Gallops” I’ve encountered on masks are derived from this record, however being pressed temporally, I’ve not had time to test.

[ad_2]